Diseases Treated | Arthritis & Autoimmune Diseases in Noida
Rheumatoid Arthritis
Ankylosing Spondylitis
Ankylosing Spondylitis

What is Rheumatoid Arthritis?
Rheumatoid arthritis is an autoimmune disorder where the immune system mistakenly attacks the synovium, the lining of the membranes that surround the joints. This leads to inflammation in the affected joints, which can eventually cause joint damage and deformities.
Symptoms
- Joint Pain: Persistent pain in the joints, especially in the morning or after periods of inactivity.
- Joint Stiffness: Morning stiffness lasting more than 30 minutes; joints may feel stiff and swollen.
- Swelling: Visible swelling around the affected joints.
- Warmth and Redness: The skin around the affected joints may be warm to the touch and appear red.
- Fatigue: General feeling of tiredness or fatigue, which can be severe.
- Loss of Joint Function: Difficulty in moving the affected joints, which can impact daily activities.
- Systemic Symptoms: Fever, loss of appetite, and weight loss may also be present.
Causes
The exact cause of RA is not fully understood, but several factors may contribute:
- Genetics: A family history of RA or other autoimmune diseases can increase risk.
- Environmental Factors: Infections, smoking, and exposure to certain chemicals may trigger the onset of RA.
- Hormonal Factors: RA is more common in women, suggesting hormones might play a role.
Diagnosis
Diagnosing RA involves a combination of clinical evaluation, laboratory tests, and imaging studies:
- Medical History and Physical Exam: Assessment of symptoms, joint examination, and review of medical history.
- Blood Tests:
- Rheumatoid Factor (RF): A protein present in many RA patients, but not exclusive to RA.
- Anti-Citrullinated Protein Antibody (ACPA): More specific to RA and can help in diagnosis.
- Erythrocyte Sedimentation Rate (ESR) or C-Reactive Protein (CRP): Indicate inflammation levels in the body.
- Imaging Studies:
- X-rays: To check for joint damage or erosion.
- Ultrasound or MRI: To assess joint inflammation and damage.
Treatment
Treatment for RA aims to reduce inflammation, manage symptoms, and prevent joint damage. It typically involves a combination of medications, physical therapy, and lifestyle changes.
Medications
- Disease-Modifying Antirheumatic Drugs (DMARDs): Methotrexate, hydroxychloroquine, sulfasalazine. These slow disease progression and prevent joint damage.
- Biologics: Target specific parts of the immune system (e.g., TNF inhibitors like adalimumab, etanercept).
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): For pain relief and inflammation reduction.
- Corticosteroids: Prednisone, used to control severe inflammation.
- Analgesics: Pain relievers like acetaminophen or stronger opioids for severe pain.
Physical Therapy
- Exercise: Low-impact exercises like swimming or walking to maintain joint function and muscle strength.
- Occupational Therapy: Techniques to help with daily activities and joint protection strategies.
Lifestyle Changes
- Diet: Anti-inflammatory diets rich in fruits, vegetables, and omega-3 fatty acids may help.
- Smoking Cessation: Smoking is a known risk factor for RA, so quitting is beneficial.
- Weight Management: Maintaining a healthy weight to reduce stress on the joints.
Ankylosing Spondylitis
Ankylosing Spondylitis
Ankylosing Spondylitis
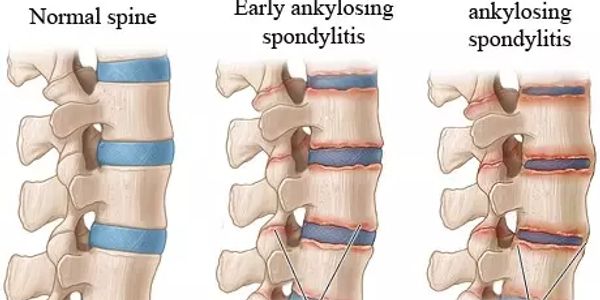
Ankylosing spondylitis (AS) is a type of inflammatory arthritis primarily affecting the spine and the sacroiliac joints (where the spine meets the pelvis). It is characterized by chronic inflammation leading to pain and stiffness in the back and can result in the fusion of the spinal vertebrae, causing a reduced range of motion. AS is part of a group of diseases known as spondyloarthritis and is considered an autoimmune disorder.
Key Features and Symptoms:
- Back Pain and Stiffness:
- Typically starts in the lower back and buttocks.
- Pain and stiffness are often worse in the morning and improve with movement.
- Chronic pain may develop over several months or years.
- Reduced Spinal Mobility:
- Gradual loss of flexibility in the spine, leading to a forward-bending posture known as "kyphosis."
- Sacroiliitis:
- Inflammation of the sacroiliac joints, which can cause pain in the lower back and buttocks.
- Peripheral Arthritis:
- Pain and swelling in other joints, such as the hips, shoulders, and knees.
- Enthesitis:
- Inflammation at the sites where tendons and ligaments attach to bones, such as the Achilles tendon or the bottom of the foot.
- Extra-Articular Symptoms:
- Eye Involvement: Uveitis or iritis, causing eye pain, redness, and sensitivity to light.
- Cardiovascular Issues: Including aortitis (inflammation of the aorta) and possible heart valve involvement.
- Pulmonary Issues: Reduced lung capacity due to rib cage involvement.
Diagnosis:
Diagnosing ankylosing spondylitis involves a combination of clinical evaluation, imaging, and laboratory tests:
- Medical History and Physical Examination:
- Assessment of symptoms, including back pain, stiffness, and any other related symptoms.
- Laboratory Tests:
- HLA-B27 Test: A genetic marker present in many people with AS, though not definitive for diagnosis. About 90% of people with AS test positive for this antigen, but not everyone with this antigen has AS.
- Inflammatory Markers: Such as erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP), which can be elevated in inflammation.
- Imaging Studies:
- X-rays: Can show changes in the spine and sacroiliac joints, such as joint space narrowing and new bone formation.
- MRI: More sensitive for detecting early inflammation and changes in the sacroiliac joints and spine.
- Bone Scintigraphy:
- A nuclear imaging technique that can be used to detect inflammation in the sacroiliac joints and spine.
Treatment:
Treatment for ankylosing spondylitis focuses on reducing inflammation, managing symptoms, and improving quality of life. Treatment strategies include:
- Medications:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): Such as ibuprofen or naproxen, to reduce pain and inflammation.
- Disease-Modifying Anti-Rheumatic Drugs (DMARDs): Like sulfasalazine, particularly useful for peripheral arthritis.
- Biologics: Target specific parts of the immune system, such as TNF-alpha inhibitors (e.g., adalimumab, infliximab) and IL-17 inhibitors (e.g., secukinumab), which are effective in managing inflammation and slowing disease progression.
- Corticosteroids: For short-term management of severe inflammation, typically used sparingly.
- Physical Therapy and Exercise:
- Stretching and Strengthening Exercises: To maintain spinal flexibility and improve posture.
- Posture Training: To counteract the forward-bending posture and promote better spinal alignment.
- Lifestyle Adjustments:
- Regular Exercise: Maintaining physical activity to improve flexibility and overall health.
- Healthy Diet: To support overall health and manage weight.
- Surgical Interventions:
- In severe cases, surgical options may be considered to correct spinal deformities or manage significant joint damage.
- Regular Monitoring:
- Ongoing evaluation by a healthcare provider to monitor disease progression and adjust treatment as necessary.
Prognosis:
The prognosis for ankylosing spondylitis varies. Some people may experience mild symptoms and maintain a relatively normal quality of life, while others may have more severe symptoms and functional limitations. Early diagnosis and treatment are crucial for managing symptoms effectively and preventing complications.
If you suspect you have ankylosing spondylitis or are experiencing symptoms, consulting a rheumatologist or a specialist in inflammatory diseases is essential for an accurate diagnosis and a comprehensive treatment plan.
Polymyalgia Rheumatica
Polymyalgia Rheumatica
Polymyalgia Rheumatica

Polymyalgia rheumatica (PMR) is an inflammatory condition that causes muscle pain and stiffness, primarily in the shoulders, hips, and neck. It often affects individuals over the age of 50 and can be associated with another condition called giant cell arteritis (GCA), which is a more serious inflammation of the blood vessels.
What is Polymyalgia Rheumatica?
Polymyalgia rheumatica is characterized by muscle pain and stiffness that typically affects the shoulders, upper arms, neck, and hips. The symptoms usually develop over a short period, and they often worsen in the morning or after periods of inactivity.
Symptoms
- Muscle Pain and Stiffness: Pain and stiffness in the shoulders, hips, and neck, especially in the morning or after rest.
- Fatigue: General feeling of tiredness and low energy.
- Fever: Low-grade fever may accompany the symptoms.
- Weight Loss: Unexplained weight loss may occur.
- Morning Stiffness: Prolonged stiffness, usually lasting more than 30 minutes after waking up.
Causes:
The exact cause of PMR is not well understood, but several factors may contribute:
- Genetics: A family history of PMR or other autoimmune conditions may increase risk.
- Age: PMR commonly affects individuals over 50, with incidence increasing with age.
- Gender: Women are more likely to develop PMR than men.
- Environmental Factors: There may be an environmental or infectious trigger, but this is not clearly defined.
Diagnosis
Diagnosing PMR involves a combination of clinical evaluation and laboratory tests:
- Medical History and Physical Examination:
- Assessment of symptoms, particularly muscle pain and stiffness in the shoulders and hips.
- Examination to rule out other conditions that might cause similar symptoms.
- Laboratory Tests:
- Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP): Elevated levels indicate inflammation.
- Rheumatoid Factor (RF) and Anti-Citrullinated Protein Antibody (ACPA): These tests help differentiate PMR from other conditions like rheumatoid arthritis.
- Imaging Studies:
- Ultrasound: Can show inflammation in the shoulder and hip joints.
- MRI: May be used to assess inflammation and rule out other conditions.
- Exclusion of Other Conditions:
- PMR is often diagnosed by ruling out other potential causes of the symptoms.
Treatment
The primary treatment for PMR is the use of corticosteroids, which are effective in reducing inflammation and alleviating symptoms:
- Corticosteroids: Prednisone is commonly used to rapidly reduce inflammation and improve symptoms. The dose is typically high initially and then tapered down gradually.
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): May be used in conjunction with corticosteroids for additional pain relief, though they are not as effective as corticosteroids for PMR.
Long-Term Management
- Regular Monitoring: Regular follow-up with a healthcare provider to monitor response to treatment and adjust medication as needed.
- Bone Health: Prolonged use of corticosteroids can impact bone health, so calcium and vitamin D supplements may be recommended.
- Lifestyle Modifications: Exercise, balanced diet, and weight management can help maintain overall health and manage symptoms.
Complications
- Giant Cell Arteritis (GCA): About 10-20% of people with PMR may develop GCA, which is a more serious condition that can cause vision problems and other complications. Immediate treatment with corticosteroids is crucial to prevent severe complications.
Prognosis
- Response to Treatment: Most people with PMR respond well to corticosteroid treatment, and symptoms typically improve within weeks.
- Relapse: Symptoms may recur, and some individuals may need ongoing treatment for an extended period.
Support and Resources
- Patient Education: Understanding the condition and treatment options can help manage PMR effectively.
- Support Groups: Connecting with others who have PMR can provide emotional support and practical advice.
- Medical Professional: Regular consultations with a rheumatologist or healthcare provider for ongoing management and monitoring
SLE
Polymyalgia Rheumatica
Polymyalgia Rheumatica

- Autoimmune Nature: In SLE, the immune system mistakenly targets healthy cells and tissues, which can lead to inflammation and damage in various parts of the body.
- Symptoms: The disease can cause a wide range of symptoms, which may vary greatly from person to person. Common symptoms include:
- Skin Rashes: Often a butterfly-shaped rash across the cheeks and nose.
- Joint Pain: Swelling and pain in joints.
- Fatigue: Persistent tiredness that doesn’t improve with rest.
- Fever: Low-grade fever without a clear cause.
- Kidney Issues: Known as lupus nephritis, which can affect kidney function.
- Heart and Lung Problems: Inflammation of the heart (pericarditis) or lungs (pleuritis).
- Diagnosis: Diagnosing SLE can be challenging as symptoms overlap with other conditions. Tests may include:
- Blood Tests: To check for specific antibodies like anti-nuclear antibodies (ANA) and anti-double-stranded DNA.
- Urinalysis: To check for kidney involvement.
- Imaging: To assess organ involvement.
- Treatment: There’s no cure for SLE, but treatments can help manage symptoms and prevent flare-ups. Common treatments include:
- Anti-inflammatory Medications: Like nonsteroidal anti-inflammatory drugs (NSAIDs) for joint pain and inflammation.
- Corticosteroids: To reduce inflammation and control severe symptoms.
- Immunosuppressants: Medications like hydroxychloroquine ,MMF,Belimumab and Rituximab to suppress the immune response.
- Prognosis: With appropriate treatment, many people with SLE can lead active and fulfilling lives. Regular monitoring and adjustments in treatment are often necessary to manage the disease effectively.
If you have any specific questions or need more details about SLE, feel free to ask!
Welcome to Srigyan Rheumatology Clinic Medical Centre
Sjogren's Syndrome
Sjogren's Syndrome
Sjogren's Syndrome

Sjogren’s syndrome is an autoimmune disorder characterized by the body's immune system attacking its own moisture-producing glands. This primarily affects the salivary glands and tear glands, leading to dryness in the mouth and eyes. It can also affect other parts of the body, including joints, skin, and internal organs.
Symptoms of Sjogren’s Syndrome:
- Dry Mouth (Xerostomia):
- Difficulty swallowing or speaking
- Increased dental cavities
- Swollen salivary glands
- Dry Eyes (Xerophthalmia):
- Burning or gritty sensation
- Redness and irritation
- Excessive tearing or eye infections
- Joint Pain and Swelling:
- Arthritis-like symptoms affecting joints
- Fatigue:
- Persistent tiredness and lack of energy
- Dry Skin:
- Itchy or rough skin
- Vaginal Dryness:
- Discomfort or pain during sexual intercourse
- Swollen Glands:
- Especially around the jaw and neck
Diagnosis:
Diagnosing Sjogren’s syndrome can be challenging as its symptoms overlap with other conditions. It usually involves:
- Medical History and Physical Examination: Discussing symptoms and checking for signs of dryness or swelling.
- Blood Tests: To check for specific antibodies, such as anti-SSA (Ro) and anti-SSB (La), and other markers of inflammation.
- Salivary Gland Biopsy: A small sample of tissue from the lip may be examined to check for inflammation.
- Eye Tests: Such as the Schirmer test to measure tear production.
- Imaging: Salivary gland imaging, like sialography or ultrasound, to assess gland function and structure.
Treatment:
There’s no cure for Sjogren’s syndrome, but treatment focuses on managing symptoms and improving quality of life:
- Medications:
- Artificial Tears: To relieve dry eyes.
- Saline Sprays or Gels: To relieve dry mouth.
- Cholinergic Agents: Such as pilocarpine or cevimeline, to stimulate saliva production.
- Anti-inflammatory Drugs: For joint pain and inflammation.
- Lifestyle Adjustments:
- Hydration: Drinking plenty of fluids and using a humidifier to help with dryness.
- Oral Care: Regular dental check-ups and using fluoride treatments to prevent cavities.
- Eye Care: Using preservative-free artificial tears and avoiding irritants.
- Management of Associated Conditions:
- Treating secondary symptoms or complications, such as arthritis or rashes.
- Regular Monitoring:
- Ongoing evaluation by healthcare providers to manage symptoms and adjust treatments as needed.
- Supportive Therapies:
- Counseling or Support Groups: To help manage the emotional impact of chronic illness.
Because Sjogren’s syndrome can affect multiple body systems, treatment often involves a multidisciplinary approach. Working closely with rheumatologists, ophthalmologists, dentists, and other specialists can help manage the condition effectively. If you suspect you have Sjogren’s syndrome or are experiencing symptoms, consulting a healthcare professional for an accurate diagnosis and personalized treatment plan is crucial.
Sarcoidosis
Sjogren's Syndrome
Sjogren's Syndrome
Sarcoidosis is an inflammatory disease characterized by the formation of small clusters of inflammatory cells, known as granulomas, in various organs of the body. The exact cause of sarcoidosis is unknown, but it is believed to be related to an abnormal immune response. The disease can affect multiple organs, but it most commonly affects the lungs and lymph nodes.
Symptoms of Sarcoidosis:
Sarcoidosis can vary widely in its presentation and severity, and symptoms may differ depending on the organs affected. Common symptoms include:
- Pulmonary Sarcoidosis (affecting the lungs):
- Persistent cough
- Shortness of breath
- Chest pain
- Fatigue
- Lymphatic Sarcoidosis (affecting lymph nodes):
- Swollen lymph nodes, especially in the chest or neck
- Skin Sarcoidosis:
- Rashes or nodules on the skin (e.g., erythema nodosum, lupus pernio)
- Skin lesions that may be red or purple
- Ocular Sarcoidosis (affecting the eyes):
- Eye redness or irritation
- Blurred vision
- Sensitivity to light
- Musculoskeletal Sarcoidosis:
- Joint pain
- Muscle pain or weakness
- Systemic Symptoms:
- Fever
- Night sweats
- Weight loss
Diagnosis of Sarcoidosis:
Diagnosing sarcoidosis can be challenging due to its wide range of symptoms and overlap with other conditions. The diagnosis often involves:
- Medical History and Physical Examination:
- Evaluating symptoms and conducting a thorough physical exam.
- Imaging Studies:
- Chest X-ray: To look for characteristic lung changes.
- CT Scan: To provide more detailed images of the chest and other organs.
- Biopsy:
- A tissue sample from an affected organ, such as the lung, skin, or lymph nodes, is examined for granulomas.
- Blood Tests:
- To check for elevated levels of markers such as angiotensin-converting enzyme (ACE) and to rule out other conditions.
- Pulmonary Function Tests:
- To assess lung function if the lungs are affected.
- Ophthalmologic Exam:
- To evaluate for eye involvement.
Treatment of Sarcoidosis:
Treatment for sarcoidosis depends on the severity of symptoms and the organs involved. Many people with sarcoidosis have mild symptoms that resolve on their own, but more severe cases may require treatment:
- Medications:
- Corticosteroids: Such as prednisone, are commonly used to reduce inflammation and manage symptoms.
- Immunosuppressive Drugs: For cases that do not respond to corticosteroids or for long-term management, drugs such as methotrexate or azathioprine may be used.
- Symptom Management:
- Pain Relief: Nonsteroidal anti-inflammatory drugs (NSAIDs) or other pain relievers for joint and muscle pain.
- Eye Drops: For managing eye symptoms.
- Monitoring and Follow-up:
- Regular check-ups to monitor disease progression and response to treatment.
- Lifestyle Adjustments:
- Healthy Lifestyle: Maintaining a balanced diet, regular exercise, and avoiding smoking can help manage symptoms and improve overall health.
- Supportive Care:
- Counseling and Support Groups: For emotional and psychological support.
Prognosis:
The prognosis for sarcoidosis varies. In many cases, the disease may resolve on its own without significant treatment. However, some people may experience chronic symptoms or complications, especially if vital organs are involved. Regular monitoring and timely treatment can help manage the condition effectively.
If you suspect you have sarcoidosis or are experiencing symptoms, it’s essential to consult a Rheumatologistl for an accurate diagnosis and an appropriate treatment plan.
Scleroderma
Sjogren's Syndrome
Behcet's Syndrome
Scleroderma, also known as systemic sclerosis, is a chronic autoimmune disease characterized by the hardening and tightening of the skin and connective tissues. It can also affect internal organs, such as the lungs, heart, kidneys, and digestive tract. Scleroderma is a complex condition that varies widely in severity and presentation.
Types of Scleroderma:
- Localized Scleroderma:
- Morphea: Characterized by thick, hardened patches of skin that may appear on one or several areas of the body.
- Linear Scleroderma: Involves lines of thickened skin, often on the arms, legs, or forehead.
- Systemic Scleroderma:
- Limited Scleroderma (CREST Syndrome): A form that affects the skin on the fingers, hands, and face, and may involve internal organs. CREST stands for Calcinosis, Raynaud's phenomenon, Esophageal dysmotility, Sclerodactyly, and Telangiectasia.
- Diffuse Scleroderma: A more aggressive form that affects a larger area of the skin and internal organs, often with rapid progression.
Symptoms of Scleroderma:
Symptoms can vary widely depending on the type and severity of the disease. Common symptoms include:
- Skin Changes:
- Thickened or hardened skin
- Tightness and swelling
- Changes in skin color
- Raynaud’s Phenomenon:
- Reduced blood flow to the fingers and toes, causing them to turn white or blue in response to cold or stress.
- Digestive Issues:
- Acid reflux
- Difficulty swallowing
- Abdominal pain and bloating
- Changes in bowel habits
- Respiratory Issues:
- Shortness of breath
- Persistent cough
- Joint and Muscle Pain:
- Swelling and stiffness in joints
- Muscle pain or weakness
- Kidney Problems:
- High blood pressure
- Kidney dysfunction
- Cardiac Symptoms:
- Irregular heartbeat
- Heart failure
Diagnosis of Scleroderma:
Diagnosing scleroderma involves a combination of clinical evaluation and diagnostic tests:
- Medical History and Physical Examination:
- Detailed assessment of symptoms and physical examination of the skin and other affected areas.
- Blood Tests:
- To check for specific autoantibodies (e.g., anti-Scl-70, anti-centromere antibodies) and markers of inflammation.
- Skin Biopsy:
- A sample of skin tissue may be examined for characteristic changes.
- Imaging Studies:
- Chest X-ray or CT Scan: To evaluate lung involvement.
- Echocardiogram: To assess heart function.
- Pulmonary Function Tests:
- To measure lung capacity and function.
- Endoscopy:
- To evaluate the digestive tract if there are gastrointestinal symptoms.
Treatment of Scleroderma:
Treatment for scleroderma focuses on managing symptoms, preventing complications, and improving quality of life:
- Medications:
- Immunosuppressants: Such as methotrexate or cyclophosphamide to control inflammation and immune response.
- Corticosteroids: For reducing inflammation in some cases.
- Antifibrotic Agents: To target fibrosis and skin thickening (e.g., nintedanib).
- Raynaud's Medications: Such as calcium channel blockers or PDE5 inhibitors for improving blood flow.
- Symptom Management:
- Skin Care: Regular moisturizing and using protective measures to manage skin symptoms.
- Digestive Aids: Medications to manage acid reflux and digestive issues.
- Pain Management: Pain relievers and physical therapy for joint and muscle pain.
- Lifestyle Adjustments:
- Healthy Diet: A balanced diet can help manage digestive symptoms and overall health.
- Regular Exercise: To maintain joint flexibility and overall well-being.
- Avoiding Triggers: Such as extreme temperatures and stress, which can exacerbate symptoms.
- Supportive Therapies:
- Occupational and Physical Therapy: To help with mobility and daily activities.
- Counseling and Support Groups: For emotional support and coping strategies.
Prognosis:
The prognosis for scleroderma varies widely. Some individuals may experience mild symptoms with minimal impact on their quality of life, while others may face more severe complications affecting multiple organs. Early diagnosis and proactive management can help improve outcomes and quality of life.
If you suspect you have scleroderma or are experiencing symptoms, consulting a healthcare professional, ideally a rheumatologist, is essential for an accurate diagnosis and a comprehensive treatment plan.
Behcet's Syndrome
Adult onset still's disease
Behcet's Syndrome
Behçet's disease is a rare, chronic autoimmune condition characterized by inflammation of blood vessels throughout the body. The exact cause of Behçet's disease is unknown, but it is believed to involve genetic, environmental, and possibly infectious factors. The disease can affect multiple organ systems and often leads to recurrent symptoms.
Key Features and Symptoms:
- Oral Ulcers:
- Painful sores or ulcers inside the mouth that can resemble canker sores. These are often one of the first symptoms and can recur frequently.
- Genital Ulcers:
- Painful sores or ulcers on the genital area, which can also recur.
- Skin Lesions:
- Erythema Nodosum: Painful, red nodules typically found on the legs.
- Papulopustular Lesions: Small, pus-filled bumps.
- Eye Problems:
- Uveitis: Inflammation of the middle layer of the eye, which can lead to pain, redness, blurred vision, and sensitivity to light.
- Retinal Vasculitis: Inflammation of the blood vessels in the retina.
- Joint Pain:
- Arthritis-like symptoms, which may involve swelling, pain, and stiffness in the joints.
- Vascular Issues:
- Inflammation of blood vessels (vasculitis) can lead to blood clots or aneurysms in severe cases.
- Neurological Symptoms:
- Headaches, confusion, and in rare cases, symptoms such as seizures or stroke-like symptoms.
- Gastrointestinal Problems:
- Abdominal pain, diarrhea, or nausea, though these are less common.
Diagnosis:
Diagnosing Behçet's disease can be challenging due to its variable presentation and the overlap with other conditions. The diagnosis is usually based on clinical criteria, including:
- Medical History and Physical Examination:
- Assessment of symptoms and physical examination to identify characteristic signs.
- Diagnostic Criteria:
- The International Study Group for Behçet's Disease has established criteria that include recurrent oral ulcers plus two of the following: recurrent genital ulcers, eye inflammation, skin lesions, or a positive pathergy test (a skin reaction to needle prick).
- Laboratory Tests:
- Blood tests to check for inflammation and rule out other conditions. Specific tests may not diagnose Behçet's but can help in the differential diagnosis.
- Pathergy Test:
- A skin test where a needle prick is observed for an exaggerated inflammatory response, which can be indicative of Behçet’s disease in some cases.
- Imaging Studies:
- Imaging such as MRI or ultrasound may be used to evaluate internal organ involvement and assess complications.
Treatment:
Treatment for Behçet's disease focuses on managing symptoms, reducing inflammation, and preventing complications:
- Medications:
- Anti-inflammatory Drugs: Nonsteroidal anti-inflammatory drugs (NSAIDs) to manage joint pain and skin lesions.
- Corticosteroids: Such as prednisone, to reduce inflammation in severe cases.
- Immunosuppressants: Drugs like azathioprine, methotrexate, or cyclosporine to suppress the immune system and manage systemic symptoms.
- Biologics: Medications such as infliximab or adalimumab may be used for severe or resistant cases.
- Colchicine: Particularly effective for managing skin and joint symptoms.
- Symptom Management:
- Eye Care: Regular monitoring and treatment by an ophthalmologist to manage eye inflammation and prevent vision loss.
- Oral Care: Topical treatments and pain relief for oral and genital ulcers.
- Pain Relief: Pain management strategies for joint pain or headaches.
- Lifestyle Adjustments:
- Healthy Lifestyle: Maintaining a balanced diet and managing stress can help manage symptoms.
- Avoiding Triggers: Identifying and avoiding potential triggers, such as certain foods or environmental factors, may help reduce flare-ups.
- Regular Monitoring:
- Regular follow-ups with healthcare providers to monitor disease progression and adjust treatment as needed.
Prognosis:
The prognosis for Behçet's disease varies widely. Some individuals may experience mild symptoms that are manageable with treatment, while others may have more severe disease with significant impact on quality of life. Early diagnosis and comprehensive management can help improve outcomes and reduce the risk of complications.
If you suspect you have Behçet's disease or are experiencing symptoms, consulting a healthcare professional, particularly a rheumatologist or a specialist familiar with autoimmune conditions, is crucial for an accurate diagnosis and a tailored treatment plan.
Adult onset still's disease
Adult onset still's disease
Adult onset still's disease
Adult-onset Still's disease (AOSD) is a rare and potentially serious systemic inflammatory condition that primarily affects adults. It is considered a type of systemic juvenile idiopathic arthritis (sJIA) but occurs after childhood. It is characterized by a combination of symptoms including fever, rash, and arthritis, and can affect multiple organs. The exact cause of AOSD is not known, but it is thought to involve genetic and environmental factors.
Key Features and Symptoms:
- Fever:
- High, spiking fevers that often occur in a daily pattern, such as every afternoon or evening. These fevers can be quite severe and are a hallmark of the disease.
- Rash:
- A salmon-colored, pink or red rash that may appear during fever spikes. The rash often comes and goes with the fever.
- Arthritis:
- Joint pain and swelling that can affect multiple joints. This may start suddenly and can be associated with morning stiffness.
- Systemic Symptoms:
- Fatigue
- Weight loss
- Muscle pain
- Organ Involvement:
- Liver: Hepatomegaly (enlarged liver) and abnormal liver function tests.
- Spleen: Splenomegaly (enlarged spleen).
- Lymph Nodes: Enlarged lymph nodes.
- Other Symptoms:
- Pharyngitis: Sore throat that may accompany the fever.
- Serositis: Inflammation of the lining of the heart (pericarditis) or lungs (pleuritis).
Diagnosis:
Diagnosing AOSD involves ruling out other conditions and confirming the presence of characteristic symptoms. The diagnostic process may include:
- Medical History and Physical Examination:
- Detailed assessment of symptoms, including fever patterns, rash, and joint symptoms.
- Laboratory Tests:
- Blood Tests: Elevated levels of inflammatory markers like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Tests may also show anemia and elevated white blood cell counts.
- Autoimmune Panels: To rule out other autoimmune diseases. Tests for specific autoantibodies (e.g., rheumatoid factor, antinuclear antibodies) are usually negative in AOSD.
- Imaging Studies:
- X-rays or Ultrasound: To assess joint damage and rule out other causes of arthritis.
- CT Scan or MRI: To evaluate internal organ involvement if needed.
- Biopsy:
- In some cases, a biopsy of affected tissues may be performed to rule out other conditions.
- Exclusion of Other Diseases:
- Infections: To rule out infectious causes of fever and rash.
- Other Autoimmune Diseases: Such as rheumatoid arthritis or systemic lupus erythematosus.
Treatment:
Treatment for AOSD aims to control inflammation, manage symptoms, and prevent complications:
- Medications:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): To reduce pain and inflammation.
- Corticosteroids: Such as prednisone, to control inflammation and manage acute symptoms.
- Disease-Modifying Anti-Rheumatic Drugs (DMARDs): Such as methotrexate or sulfasalazine, may be used for chronic disease management.
- Biologics: Medications such as tocilizumab or anakinra may be used in severe or refractory cases.
- Symptom Management:
- Pain Relief: Analgesics or physical therapy to manage joint pain and stiffness.
- Monitoring and Management of Complications: Regular follow-up to assess organ involvement and adjust treatment as needed.
- Lifestyle Adjustments:
- Healthy Diet and Exercise: To support overall health and manage symptoms.
- Stress Management: Techniques to help cope with the chronic nature of the disease.
Prognosis:
The prognosis for AOSD varies. Some individuals may respond well to treatment and experience periods of remission, while others may have persistent symptoms or complications. Early diagnosis and treatment are crucial for managing the disease effectively and improving quality of life.
If you suspect you have adult-onset Still's disease or are experiencing symptoms, it’s important to consult a healthcare professional, particularly a rheumatologist, for an accurate diagnosis and a personalized treatment plan.
Psoriasis
Adult onset still's disease
Adult onset still's disease
Psoriasis is a chronic autoimmune skin condition characterized by the rapid turnover of skin cells, leading to thick, scaly patches of skin. It is an inflammatory disease that primarily affects the skin but can also involve joints and, in some cases, other organs. While there is no cure for psoriasis, various treatments can help manage symptoms and improve quality of life.
Types of Psoriasis
- Plaque Psoriasis:
- The most common type, characterized by dry, raised, red skin lesions (plaques) covered with thick, silvery scales. These plaques often appear on the scalp, elbows, knees, and lower back.
- Nail Psoriasis:
- Affects the nails, causing pitting, abnormal nail growth, discoloration, and in severe cases, nail loss.
- Guttate Psoriasis:
- Often starts in childhood or young adulthood and appears as small, water-drop-shaped, scaling lesions on the trunk, arms, legs, and scalp. It can be triggered by infections, particularly streptococcal throat infections.
- Inverse Psoriasis:
- Causes bright red, shiny, and inflamed skin around the genitals, buttocks, or other folds of the body. It often appears in skin folds where sweat and friction can be common.
- Pustular Psoriasis:
- Characterized by white pustules (blisters of noninfectious pus) surrounded by red skin. It can be localized (on the hands or feet) or generalized (covering large areas of the body).
- Erythrodermic Psoriasis:
- The least common type, covering large areas of the body with a red, peeling rash that can itch or burn. It can be severe and may require hospitalization.
Symptoms
Symptoms of psoriasis can vary widely but generally include:
- Red Patches of Skin: Covered with silvery-white scales.
- Itching and Burning: Common around affected areas.
- Dry, Cracked Skin: That may bleed.
- Joint Pain: In cases where psoriasis affects the joints, known as psoriatic arthritis.
- Nail Changes: Such as pitting, discoloration, and separation from the nail bed.
Causes and Triggers
Psoriasis is thought to be caused by an immune system dysfunction that speeds up skin cell growth. Factors that may trigger or worsen psoriasis include:
- Genetics: A family history of psoriasis increases the risk.
- Infections: Especially streptococcal throat infections.
- Stress: Can exacerbate symptoms.
- Injury to the Skin: Such as cuts, sunburns, or bug bites (known as Koebner phenomenon).
- Medications: Certain drugs can trigger or worsen psoriasis.
- Lifestyle Factors: Smoking and excessive alcohol consumption.
Diagnosis
Diagnosing psoriasis typically involves:
- Medical History and Physical Examination: Evaluation of symptoms and appearance of the skin.
- Skin Biopsy: In some cases, a small sample of skin may be taken and examined under a microscope to confirm the diagnosis and differentiate it from other skin conditions.
- Blood Tests: Not usually necessary for diagnosis but may be used to rule out other conditions.
Treatment
Treatment for psoriasis aims to reduce inflammation, control symptoms, and improve quality of life. Options include:
- Topical Treatments:
- Corticosteroids: To reduce inflammation and itching.
- Vitamin D Analogues: Such as calcipotriene, to slow skin cell growth.
- Coal Tar: To reduce scaling and itching.
- Topical Calcineurin Inhibitors: Like tacrolimus or pimecrolimus, especially useful in sensitive areas.
- Phototherapy:
- UVB Therapy: Exposing the skin to ultraviolet B light to reduce symptoms.
- PUVA Therapy: Combines a drug called psoralen with UVA light to treat more severe cases.
- Systemic Treatments:
- Oral Medications: Such as methotrexate, cyclosporine, or acitretin to reduce inflammation and slow skin cell growth.
- Biologics: Injectables that target specific parts of the immune system, such as TNF-alpha inhibitors (e.g., adalimumab), IL-12/23 inhibitors (e.g., ustekinumab), and IL-17 inhibitors (e.g., secukinumab).
- Lifestyle and Home Remedies:
- Moisturizers: To prevent skin dryness and scaling.
- Baths: With oatmeal or Epsom salts to soothe the skin.
- Healthy Diet: Avoiding triggers and eating a balanced diet.
- Stress Management: Techniques to manage stress can help reduce flare-ups.
- Regular Monitoring:
- Ongoing follow-up with a healthcare provider to monitor disease progression and treatment effectiveness.
Prognosis
Psoriasis is a chronic condition with no cure, but many people can manage their symptoms effectively with appropriate treatment. The severity of the disease varies from person to person, and treatment plans are often adjusted based on how well symptoms are controlled and the impact on daily life.
Polymyositis
Autoimmune Necrotizing Myopathy
Anti-Synthetase Syndrome
Polymyositis is a rare autoimmune disease characterized by chronic inflammation and weakness of the skeletal muscles. It is part of a group of disorders known as idiopathic inflammatory myopathies. Polymyositis primarily affects adults, though it can occur at any age. The exact cause of polymyositis is not well understood, but it is believed to involve an autoimmune response where the body’s immune system attacks its own muscle tissues.
Key Features and Symptoms:
- Muscle Weakness:
- Symmetrical Muscle Weakness: Typically affects the proximal muscles, such as those in the shoulders, hips, and thighs, leading to difficulty with activities like climbing stairs, lifting objects, or raising arms.
- Progressive Weakness: Symptoms usually develop gradually over weeks or months.
- Muscle Pain and Discomfort:
- Some people may experience muscle pain or tenderness, though it is less common than weakness.
- Fatigue:
- General fatigue and feeling of tiredness, often exacerbated by muscle use.
- Dysphagia:
- Difficulty swallowing due to weakness in the muscles of the throat.
- Respiratory Symptoms:
- In severe cases, weakness in the respiratory muscles can lead to shortness of breath.
Diagnosis:
Diagnosing polymyositis involves a combination of clinical evaluation, laboratory tests, and imaging studies:
- Medical History and Physical Examination:
- Assessment of symptoms, muscle strength, and physical examination to identify characteristic signs of muscle weakness.
- Laboratory Tests:
- Muscle Enzymes: Elevated levels of muscle enzymes such as creatine kinase (CK) and aldolase in the blood can indicate muscle damage.
- Autoantibodies: Tests for specific autoantibodies, such as anti-Jo-1, can support the diagnosis, though they are not always present.
- Electromyography (EMG):
- A test that measures electrical activity in the muscles, which can show characteristic changes in polymyositis.
- Muscle Biopsy:
- A sample of muscle tissue is taken and examined under a microscope for signs of inflammation and muscle damage. This is considered a key diagnostic test for confirming polymyositis.
- Magnetic Resonance Imaging (MRI):
- MRI of the muscles can help detect inflammation and guide muscle biopsy.
- Other Tests:
- Chest X-ray or CT Scan: To check for any lung involvement if there are respiratory symptoms.
Treatment:
Treatment for polymyositis focuses on reducing inflammation, improving muscle strength, and managing symptoms:
- Medications:
- Corticosteroids: Such as prednisone, are the primary treatment to reduce inflammation and muscle weakness.
- Immunosuppressants: Drugs like methotrexate or azathioprine may be used in conjunction with corticosteroids for cases that are resistant to treatment or to reduce corticosteroid dosages.
- Biologics: In severe cases, medications such as rituximab may be considered.
- Physical Therapy and Exercise:
- Rehabilitation: A tailored exercise program to maintain muscle strength and function. Physical therapy can also help improve mobility and reduce the risk of muscle contractures.
- Lifestyle Adjustments:
- Dietary Changes: Ensuring adequate nutrition to support overall health and muscle function.
- Rest and Avoiding Overexertion: Balancing activity with rest to prevent muscle strain and fatigue.
- Regular Monitoring:
- Ongoing follow-up with a healthcare provider to monitor disease progression and adjust treatment as needed.
Prognosis:
The prognosis for polymyositis varies. Some individuals may respond well to treatment and experience significant improvement in muscle strength and function. Others may have persistent symptoms or complications. Early diagnosis and treatment are crucial for managing the disease effectively and improving outcomes.
If you suspect you have polymyositis or are experiencing symptoms, consulting a rheumatologist or a specialist in autoimmune diseases is essential for an accurate diagnosis and an individualized treatment plan.
Anti-Synthetase Syndrome
Autoimmune Necrotizing Myopathy
Anti-Synthetase Syndrome
Anti-synthetase syndrome is a subset of autoimmune diseases characterized by the presence of specific autoantibodies called anti-synthetase antibodies. This syndrome is associated with a group of conditions known as idiopathic inflammatory myopathies, which include polymyositis and dermatomyositis. The syndrome features a combination of symptoms and clinical manifestations that reflect autoimmune inflammation affecting multiple organ systems.
Key Features and Symptoms:
- Muscle Involvement:
- Myositis: Muscle inflammation leading to weakness, particularly in the proximal muscles (shoulders, hips, and thighs).
- Muscle Pain: Some patients may experience muscle tenderness.
- Interstitial Lung Disease (ILD):
- Pulmonary Fibrosis: Progressive lung scarring leading to symptoms such as shortness of breath, dry cough, and reduced exercise tolerance.
- Ground-glass opacities: Seen on imaging studies, indicative of inflammation in the lungs.
- Arthritis:
- Joint pain and swelling, which may be present in addition to or instead of muscle symptoms.
- Raynaud’s Phenomenon:
- Color Changes: Fingers or toes turning white or blue in response to cold or stress, followed by redness as they warm up.
- Skin Manifestations:
- Though less common, some patients may have skin rashes similar to those seen in dermatomyositis, such as heliotrope rash or Gottron's papules.
- Fever and Fatigue:
- General feelings of fatigue and sometimes intermittent fevers.
Diagnosis:
Diagnosing anti-synthetase syndrome involves a combination of clinical evaluation, laboratory tests, and imaging studies:
- Medical History and Physical Examination:
- Detailed assessment of symptoms, including muscle weakness, respiratory issues, and joint pain.
- Laboratory Tests:
- Anti-Synthetase Antibodies: Presence of specific autoantibodies such as anti-Jo-1 (the most common), anti-PL-7, anti-PL-12, anti-EJ, anti-OJ, and others.
- Muscle Enzymes: Elevated levels of muscle enzymes such as creatine kinase (CK) and aldolase can indicate muscle damage.
- Electromyography (EMG):
- To evaluate electrical activity in the muscles and detect characteristic changes of muscle inflammation.
- Muscle Biopsy:
- A sample of muscle tissue is taken and examined under a microscope to confirm the diagnosis of myositis and rule out other conditions.
- Imaging Studies:
- Chest X-ray or CT Scan: To assess lung involvement and detect interstitial lung disease.
- Pulmonary Function Tests:
- To evaluate lung function and assess the extent of respiratory impairment.
Treatment:
Treatment for anti-synthetase syndrome focuses on managing inflammation, improving muscle strength, and addressing complications. Strategies include:
- Medications:
- Corticosteroids: Such as prednisone, to reduce inflammation and muscle weakness.
- Immunosuppressants: Drugs like methotrexate, azathioprine, or mycophenolate mofetil to help control symptoms and reduce reliance on corticosteroids.
- Biologics: In severe cases, medications like rituximab or tocilizumab may be used to target specific parts of the immune system.
- Physical Therapy and Exercise:
- Rehabilitation: Tailored exercise programs to maintain muscle strength, flexibility, and overall function. Physical therapy can also help with managing fatigue and improving quality of life.
- Respiratory Care:
- Management of Interstitial Lung Disease: This may include medications to control lung inflammation, and in severe cases, oxygen therapy or other supportive measures.
- Lifestyle Adjustments:
- Regular Monitoring: Frequent follow-up with healthcare providers to monitor disease progression and adjust treatment as needed.
- Healthy Lifestyle: Including a balanced diet, avoiding smoking, and managing stress.
Prognosis:
The prognosis for anti-synthetase syndrome varies depending on the severity of symptoms, the extent of organ involvement, and the response to treatment. Early diagnosis and comprehensive management are crucial for improving outcomes and reducing the risk of complications.
If you suspect you have anti-synthetase syndrome or are experiencing related symptoms, consulting a rheumatologist or a specialist in autoimmune diseases is essential for an accurate diagnosis and effective treatment plan.
Autoimmune Necrotizing Myopathy
Autoimmune Necrotizing Myopathy
Autoimmune Necrotizing Myopathy
Autoimmune necrotizing myopathy (AINM) is a rare but severe form of inflammatory muscle disease characterized by muscle fiber necrosis without significant inflammation. It is part of a broader category of idiopathic inflammatory myopathies, similar to polymyositis and dermatomyositis, but with distinct pathological features.
Key Features and Symptoms:
- Muscle Weakness:
- Progressive weakness of proximal muscles (those closest to the trunk), such as the shoulders, hips, and thighs. This weakness can impact daily activities like climbing stairs, lifting objects, and getting up from a seated position.
- Muscle Pain:
- While muscle pain can occur, it is not as prominent as in some other types of myopathy. The primary symptom is weakness.
- Fatigue:
- Generalized fatigue and tiredness, which may worsen with muscle use.
- Difficulty Swallowing:
- In some cases, weakness of the throat muscles may lead to dysphagia (difficulty swallowing).
- Respiratory Issues:
- In severe cases, weakness of the respiratory muscles can cause shortness of breath.
Diagnosis:
Diagnosing autoimmune necrotizing myopathy involves a combination of clinical evaluation, laboratory tests, and imaging studies:
- Medical History and Physical Examination:
- Assessment of symptoms, including muscle weakness and pain, as well as any associated features.
- Laboratory Tests:
- Muscle Enzymes: Elevated levels of muscle enzymes such as creatine kinase (CK) and aldolase indicate muscle damage.
- Autoantibodies: Specific autoantibodies associated with ANM, such as anti-SRP (signal recognition particle) and anti-HMGCR (3-hydroxy-3-methylglutaryl-CoA reductase), may be present.
- Electromyography (EMG):
- Measures electrical activity in the muscles. EMG findings in ANM may show myopathic changes with minimal inflammation.
- Muscle Biopsy:
- A key diagnostic test where a sample of muscle tissue is examined under a microscope. ANM is characterized by muscle fiber necrosis with minimal inflammatory infiltrates. This differentiates it from other inflammatory myopathies that show significant inflammation.
- Magnetic Resonance Imaging (MRI):
- MRI of the muscles can be used to assess the extent of muscle involvement and guide biopsy.
Treatment:
Treatment for autoimmune necrotizing myopathy focuses on reducing muscle inflammation, improving muscle strength, and managing symptoms. Strategies include:
- Medications:
- Corticosteroids: Such as prednisone, to reduce inflammation and muscle damage.
- Immunosuppressants: Drugs like methotrexate, azathioprine, or mycophenolate mofetil may be used to control symptoms and reduce the need for corticosteroids.
- Biologics: In cases resistant to standard treatments, medications like rituximab may be considered.
- Physical Therapy and Exercise:
- Rehabilitation: A tailored exercise program to maintain muscle strength and function. Physical therapy can also help with managing fatigue and improving quality of life.
- Lifestyle Adjustments:
- Balanced Diet: Ensuring adequate nutrition to support muscle health.
- Regular Monitoring: Frequent follow-up with healthcare providers to monitor disease progression and adjust treatment as necessary.
- Supportive Care:
- Management of Complications: Addressing any complications such as respiratory issues or swallowing difficulties.
Prognosis:
The prognosis for autoimmune necrotizing myopathy can vary. Some individuals may respond well to treatment and experience significant improvement in muscle strength and function, while others may have persistent symptoms or complications. Early diagnosis and a comprehensive treatment plan are crucial for managing the disease effectively and improving outcomes.
If you suspect you have autoimmune necrotizing myopathy or are experiencing symptoms, consulting a rheumatologist or a specialist in inflammatory muscle diseases is essential for an accurate diagnosis and an individualized treatment plan.